
You are the pediatric ID fellow on call and receive an overnight page about an infant born to a mother with HIV. Where do you start?!
What are the initial questions you should be asking?
You want to understand the maternal HIV diagnosis and management history to help understand the newborn’s risk
- History and timing of maternal HIV diagnosis and other pertinent medical history
- Was HIV diagnosis known prior to pregnancy?
- Or identified during pregnancy? If so, which trimester? Is there any concern for acute HIV infection?
- Other sexually transmitted infections that may impact pregnancy?
- Maternal HIV treatment and virologic response
- Was ART started prior to or during pregnancy? Which medication regimen?
- What is mom’s most recent viral load? What has been the recent trend in VL during pregnancy?
- Any issues with adherence?
- Intrapartum details
- Mom’s viral load (VL) near time of delivery?
- Mode of delivery?
- Any issues or complications during labor and delivery?

How do you use this information to think about the risk of HIV acquisition for this infant?
In general, a low risk scenario is a mother who has known HIV, is adherent with ART, and remains virally suppressed. There is a spectrum of what would be considered higher risk, and that risk is largely driven by the maternal viral load.
Low risk features include:
- Maternal viral suppression (HIV RNA<50) near delivery
- Mother on ART in pregnancy
- No adherence concerns
Risk of perinatal transmission less than 1%
High risk features include:
- Maternal ART concerns
- Did not receive antepartum or intrapartum ART
- Received only intrapartum ARV drugs
- Received antepartum and intrapartum ARV drugs but did not achieve viral suppression near delivery (defined as confirmed HIV RNA level <50 copies/mL within 4 weeks of delivery)
- Acute or primary infection during pregnancy (**highest risk scenario**) or breastfeeding
Risk of perinatal transmission is upwards of 25-40% in the highest risk scenarios (including whole period of time with pregnancy through breastfeeding). This is a spectrum though that is driven by maternal VL, and a mother with a VL of 50-200 copies is different than a mother with a highly elevated VL or acute HIV.
Now that you have gathered information about the case, the caller first wants to know what tests to send from the newborn?
- Virologic assays (HIV RNA or HIV DNA nucleic acid tests) that directly detect HIV must be used for diagnosis in infants and children <18 months
- Antigen/antibody immunoassays for HIV-½ and HIV-1 p24 Ag should not be used in infants!! The median age of seroreversion is 13.9 month, but 14% of infants remain seropositive after 18 months, 4.3% after 21 months, and 1.2% after 24 months (Red Book HIV Diagnostic Tests Section)
- RNA or DNA are equally recommended. DNA PCR detects proviral DNA while HIV tests measure viral RNA in plasma, so there is potential for DNA testing to be more sensitive in infants with very low viral loads — but studies have shown RNA and DNA NATs to produce comparable results
- Children should have a CBC/diff and ALT with baseline evaluation
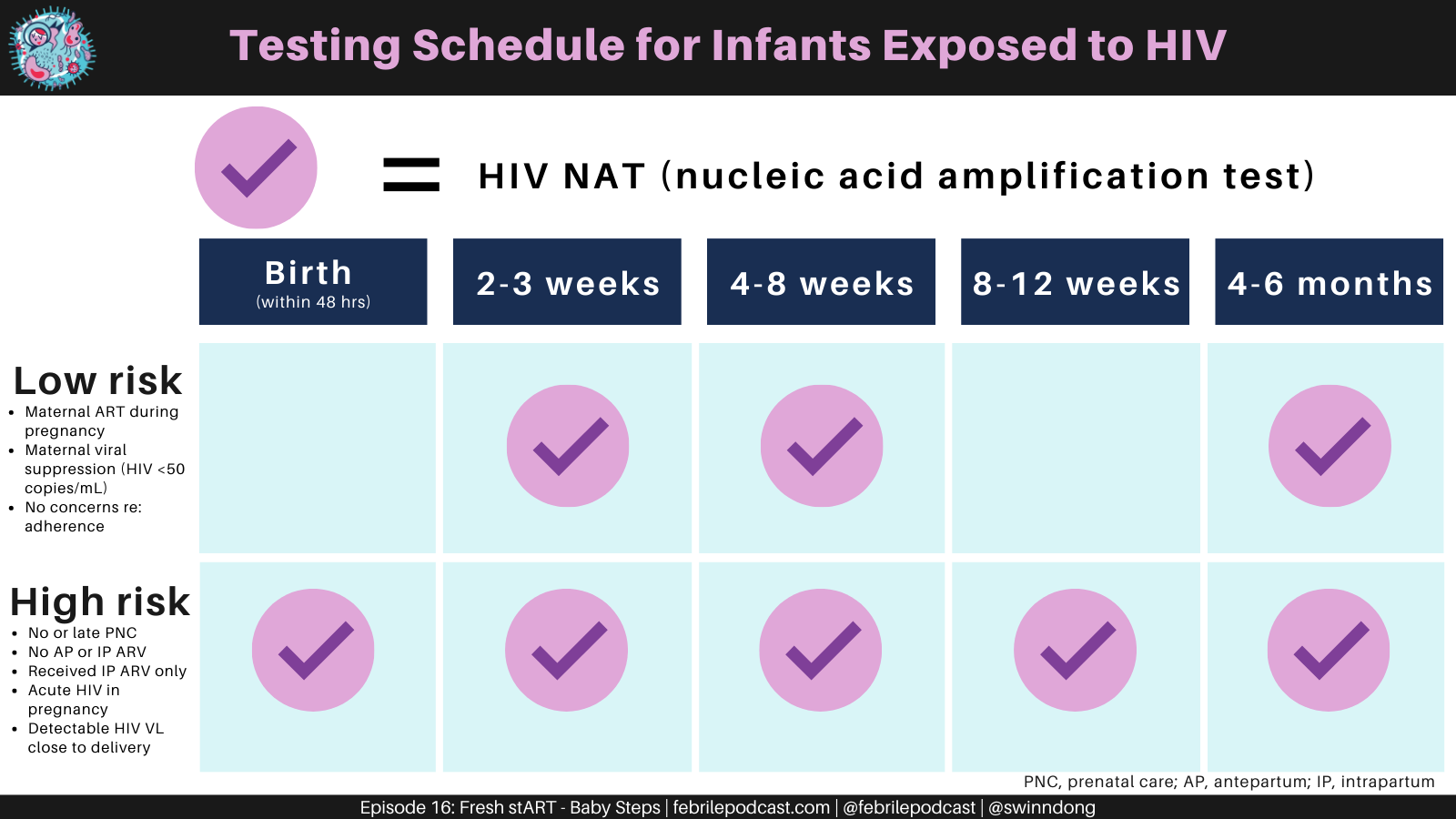
- Testing recommendations will vary based on whether the infant is low risk or high risk and include HIV NAT at following times:
- Low risk: 2-3 wks, 4-8 wks, 4-6 mo
- High risk: at birth (within 48 hrs), 2-3 wks, 4-8 wks, 2-6 wks after ARV drugs are stopped, 4-6 mo
- So high risk infants receive two additional tests: HIV NAT at birth to assess for infection in utero and a test a few weeks after stopping therapy
- The birth test has the advantage of early detection (which helps reduce loss to follow-up), but it’s disadvantages are that it can be relatively insensitive (38-57% in first 2-3 days) and a negative result is falsely reassuring.
Next the team wants to know how to treat the baby?
- Check out the US DHHS Perinatal HIV clinical guidelines for reference, but here is some general information to get started
- All newborns exposed perinatally to HIV should receive postpartum ARV drugs to reduce risk of perinatal transmission
- Newborn ART regimens should be dosed appropriately for infant gestational age and ideally will be started as close to birth as possible, preferably within 6 hrs of delivery
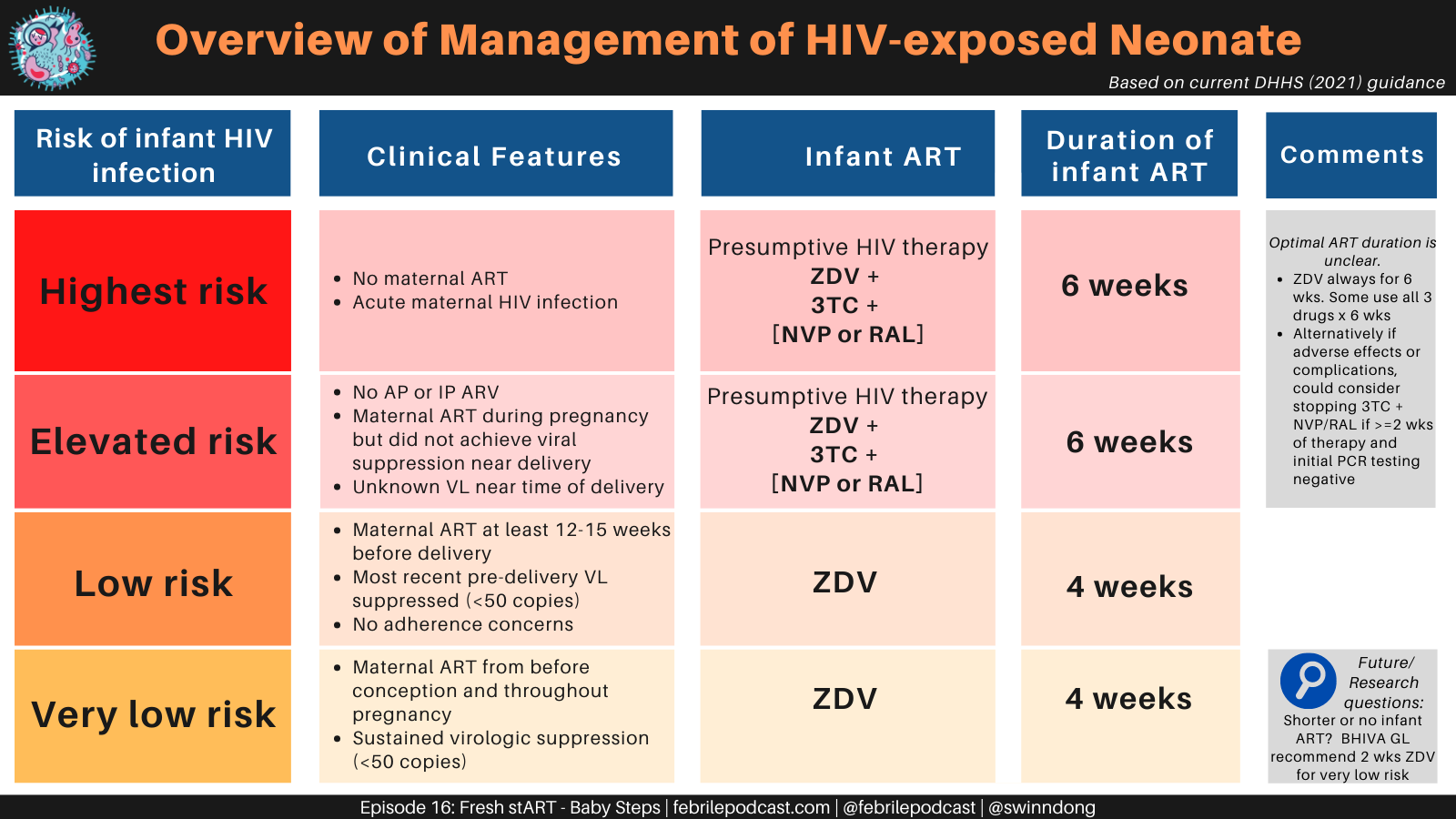
- The ART regimen will be determined based on maternal and infant factors, and you can see a guide based on the DHHS guidelines in the graphic below
- Presumptive HIV therapy is given to infants at highest risk of perinatal HIV transmission (see above section about risk) and includes:
- Zidovudine (ZDV)
- Lamivudine (3TC)
- Nevirapine (NVP) OR Raltegravir (RAL)
- A 4-week zidovudine ARV prophylaxis course can be used in newborns of moms who were virally suppressed at delivery and are low risk of perinatal HIV transmission
Key resources:
- The US DHHS (Department of Health and Human Services) Guidelines at https://clinicalinfo.hiv.gov/en/guidelines >> specifically in this scenario: Perinatal HIV clinical guidelines, Pediatric ARV clinical guidelines
- The National Clinician Consultation Center is a federally funded service that has different hotlines and resources for HIV care, perinatal HIV consultation, and other subjects (including PrEP/PEP). They provide free consultation to providers caring for women with HIV and their infants
- You can reach the perinatal HIV consultation hotline at 1-(888)-448-8765 or check their website here as well
- Want to take a deeper dive into some of the evidence? The PACTG 076 (Pediatric AIDS Clinical Trials Group) paper is the landmark efficacy trial that established the use of ARV prophylaxis with a ZDV regimen (mothers given ZDV alone during pregnancy, intrapartum period, and to their infants). It demonstrated reduction in perinatal transmission by 67.5% when compared to placebo.
- Check out the Febrile podcast episode and Consult Notes from Episode 16: Fresh StART – Baby Steps for more learning from Dr. Leslie Enane at Riley Children’s!
Uploaded on 7/18/2022
One Response
Thanks! This was a helpful post!